Table of contents
Shoulder dystocia—often mistakenly searched as shoulder dysplasia—is a birth complication where a baby’s head is delivered, but one or both shoulders get stuck behind the mother’s pubic bone. It is an obstetric emergency requiring immediate medical maneuvers to safely deliver the baby and prevent injury.
What is Shoulder Dystocia (Often Searched as Shoulder Dysplasia)?
Clarifying the Terminology: Dystocia vs. Dysplasia
Many expecting parents search for the term “shoulder dysplasia” when researching birth complications, but the correct medical term is shoulder dystocia. “Dysplasia” generally refers to abnormal cell growth or joint formation (such as hip dysplasia). “Dystocia,” on the other hand, translates to “difficult labor.”
What Happens During Delivery
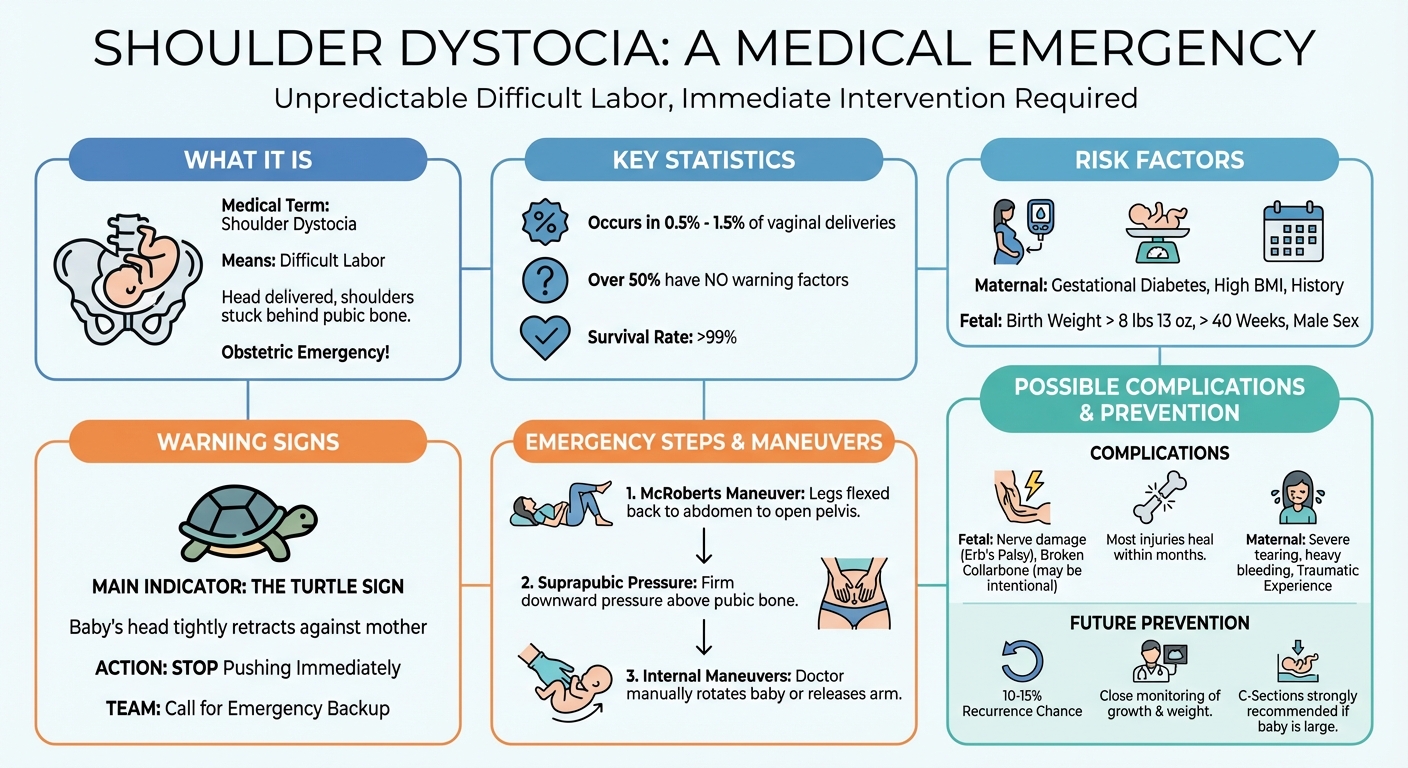
Shoulder dystocia is a specific, urgent complication that occurs during a vaginal delivery. It happens when the baby’s head successfully passes through the birth canal, but one or both of their shoulders become physically stuck behind the mother’s pubic bone. This prevents the baby’s body from following the head, halting the delivery and requiring immediate medical intervention.
How common is shoulder dysplasia in birth?
Shoulder dystocia (often mistakenly called shoulder dysplasia) is relatively rare. It occurs in approximately 0.5% to 1.5% of all vaginal deliveries. While it is an uncommon obstetric emergency, healthcare providers are extensively trained to recognize and manage it quickly to ensure a safe delivery.
Causes and Key Risk Factors
While shoulder dystocia can happen to anyone, certain factors increase the likelihood of a baby’s shoulder becoming trapped during birth.
| Maternal Risk Factors | Fetal Risk Factors |
|---|---|
| Gestational diabetes | Macrosomia (birth weight over 8 lbs 13 oz) |
| High BMI or excessive pregnancy weight gain | Post-term pregnancy (past 40 weeks) |
| History of shoulder dystocia in prior births | Male fetus (tend to be slightly larger) |
Why It Can Happen Without Warning
Despite knowing the risk factors, shoulder dystocia is largely unpredictable. Over half of all cases occur in pregnancies where no risk factors are present. Ultrasounds late in pregnancy can estimate fetal weight, but they are notoriously imprecise, meaning doctors must always be prepared for this emergency during any vaginal birth.
Warning Signs During Delivery: The Turtle Sign
How Doctors Identify the Complication
The most distinct clinical indicator of shoulder dystocia is known as the “turtle sign.” After the baby’s head is delivered, it tightly retracts back against the mother’s perineum, resembling a turtle pulling its head back into its shell. This signals that the anterior shoulder is caught on the pelvic bone.
The Immediate Medical Response
Once the turtle sign is observed, the delivery room atmosphere changes rapidly. The medical team will instruct the mother to stop pushing, as pushing can further wedge the shoulder. The delivering physician or midwife will immediately call for backup nurses, an anesthesiologist, and a pediatrician, and begin specific physical maneuvers.
Emergency Maneuvers: How Doctors Treat Shoulder Dystocia
Doctors follow a strict, step-by-step protocol of maneuvers designed to alter the mother’s pelvis shape or rotate the baby to free the trapped shoulder.
- The McRoberts Maneuver: The mother’s legs are sharply flexed back toward her abdomen. This flattens the lower spine and opens the pelvis, resolving up to 42% of cases on its own.
- Suprapubic Pressure: A nurse applies firm, downward CPR-like pressure directly on the mother’s lower abdomen (just above the pubic bone) to push the baby’s shoulder down and slip it under the bone.
- Internal Maneuvers: If external methods fail, the doctor may reach inside the birth canal to manually rotate the baby (Woods’ corkscrew maneuver) or gently grasp and deliver the baby’s posterior arm to create more room.
Can a baby survive shoulder dystocia?
Yes, the vast majority of babies survive shoulder dystocia without long-term health issues. Because it is a known obstetric emergency, medical teams use specific, rapid maneuvers to safely dislodge the baby’s shoulder. Prompt medical intervention typically prevents severe oxygen deprivation, ensuring the baby survives the delivery safely.
What is the survival rate of shoulder dystocia?
The survival rate of shoulder dystocia is extremely high, exceeding 99%. While it is a serious medical emergency that requires immediate intervention, fatal outcomes are exceptionally rare. Most complications involve temporary nerve injuries or fractures rather than life-threatening risks, provided the medical team acts swiftly.
Potential Injuries and Complications
Because the umbilical cord is compressed while the baby is stuck, time is of the essence. While most babies recover fully, the physical force required to resolve the dystocia can cause injuries.
Brachial Plexus Injuries (Erb’s Palsy)
The most common fetal injury is damage to the brachial plexus—the network of nerves running from the neck to the arm. Stretching these nerves can cause weakness or paralysis in the affected arm (Erb’s Palsy). Fortunately, most brachial plexus injuries heal completely within a few months.
Fetal Fractures
To free the baby, the collarbone (clavicle) or upper arm bone (humerus) may fracture. Sometimes, a doctor will intentionally break the clavicle to collapse the shoulder width and save the baby’s life. These fractures typically heal quickly and without long-term issues.
Maternal Complications
Mothers are also at risk for physical complications, including severe perineal tearing (3rd or 4th-degree tears), postpartum hemorrhage (heavy bleeding), and uterine rupture in rare cases.
Is shoulder dystocia considered a traumatic birth?
Yes, shoulder dystocia is widely considered a traumatic birth experience. The sudden shift from a routine delivery to a high-stress medical emergency can cause severe emotional distress, anxiety, and physical injuries for the mother. Many parents benefit from postpartum counseling to process the trauma of the event.
Prevention and Planning for Future Pregnancies
Assessing Risks for Subsequent Births
If you have experienced shoulder dystocia in a previous pregnancy, your risk of it happening again is higher (estimated between 10% and 15%). Your OB-GYN will closely monitor fetal growth via ultrasound in the third trimester and carefully manage any maternal weight gain or gestational diabetes.
When a C-Section is Recommended
To prevent a recurrence, your doctor may recommend an elective Cesarean section (C-section). This is especially common if the estimated fetal weight is over 4,500 grams (9 lbs 14 oz) in a mother with gestational diabetes, or over 5,000 grams (11 lbs) in a mother without diabetes.